Cataract Surgery
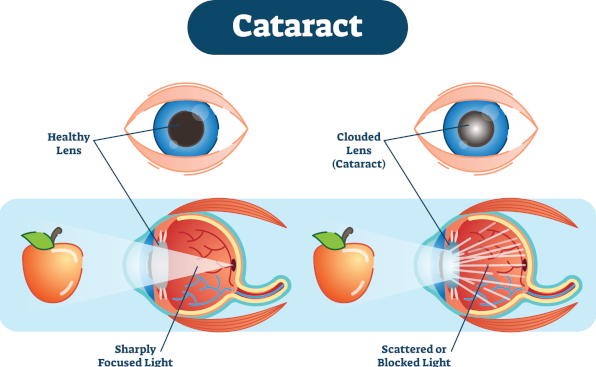
The onset of cataracts affects millions of people every year, especially adults over 60 years of age. The term cataract refers to the clouding of the natural lens of the eye due to the accumulation of oxidized proteins. Cataracts can occur in one or both eyes. Without treatment cataracts worsen over time and can lead to permanent vision loss or even blindness.

The natural lens of the eye is responsible for the refraction of light entering the eye, so that it focuses properly on the retina and ensures clear vision. Cataract means that the natural lens is cloudy and the images look blurry, yellowish or faded. Cataract surgery removes the cloudy natural lens and replaces it with a clean intraocular lens to improve your vision.
Causes of Cataracts
The natural lens of the eye gets cloudy as we grow older, causing a gradual decrease in vision. In addition to age, there are other causes of cataracts, such as:
- Trauma
- Medication use (e.g. steroids)
- Certain systemic diseases
- Diabetes
- Alcohol use
- Chronic exposure to the sun or ultraviolet (UV) radiation without sunglasses
- Smoking
- Family history of cataract
- Exposure to iatrogenic radiation in the upper body
- Other intraocular surgery (e.g. retinal detachment repair)
Most age-related cataracts develop gradually. Other cataracts, such as in young people after trauma or in people with diabetes, may develop more quickly. Regardless of the underlying cause, there is no way to predict how quickly the cataract will develop in each one of us.
Prevention
Although it is not possible to prevent cataract formation, we can certainly delay its development by taking some precautionary measures, such as:
- Wearing a wide-brimmed hat that blocks out sunlight when outdoors
- Wearing sunglasses that block ultraviolet (UV) radiation
- Quitting smoking
- Consuming green leafy vegetables, fruits and foods high in antioxidants in our daily diet
Symptoms

Cataracts affect more than 50% of adults over 60 years of age by causing progressive, painless vision loss. The classic symptoms of cataract formation are:
- Blurred vision
- Sensitivity to the reflection of lights, especially when driving at night
- Sense of cloudy vision
- Colors that appear faded
- Vision with a yellow hue
- Temporary improvement of near vision
- Double vision
- Poor night vision
- Frequent changes in the prescription of glasses or contact lenses
Diagnosis

Diagnosis requires a complete ophthalmological examination. This includes dilation of the pupils and examination of the fundus.
At first, the visual acuity is measured and refraction is performed. Each eye is tested separately for the ability to see numbers or letters of different sizes. Then, Dr. Palioura will examine the eyelids, the conjunctiva, the cornea, the iris, the anterior chamber and the lens using a slit lamp, i.e. a special microscope with a lamp and slits of certain thickness that facilitate the detection of abnormalities.
Finally, when your pupils are dilated, Dr. Palioura will examine the other organs inside the eye. Using the slit lamp again and a special ophthalmoscope (indirect ophthalmoscope), she will examine if there is a cataract and to what extent. She will then examine the vitreous, the optic nerve, the macula, the vascular network and the retinal periphery. Depending on the findings, specialized examinations such as optical coherence tomography, corneal topography or visual fields may also be needed.
Management
Early cataracts can often be observed and/or treated with non-surgical methods such as:
- New glasses prescription
- Anti-glare sunglasses
- Magnifier
- Use of brighter lighting, especially when reading

When diagnosed with early cataracts, follow these tips:
- Get an eye exam every year if you are over 65 or every two years if you are younger.
- Protect your eyes from ultraviolet sunlight by wearing sunglasses and a hat.
- If you smoke, quit smoking. Smoking is a major risk factor for cataracts.
- Use brighter lighting for reading. A magnifying glass may also be useful.
- Limit night driving if you are bothered by reflections from the incoming car lights.
- If you have diabetes, it is important that your blood sugar is well controlled.
- Use glasses with the correct prescription to improve your vision.
When cataracts begin to affect the ability to read, work or other daily activities, cataract surgery is recommended.
Modern Cataract Surgery

Modern cataract surgery is minimally invasive and replaces the cloudy natural lens of the eye (cataract) with a clear artificial lens, known as an intraocular lens. It does not require hospitalization, general anesthesia or anesthetic injection behind the eye.
Dr. Palioura performs minimally invasive cataract surgery, known as phacoemulsification. She uses topical anesthesia in the form of eye drops and small incisions that are self-sealing and do not require sutures.
Before the Surgery
The surgeon Dr. Palioura will perform special measurements to determine the power of the intraocular lens you will need. She will also ask you about the medications you are taking, and you may be asked not to take some or all of them before the surgery.
On the Day of Surgery
You will be asked to avoid eating solid food for at least 6-8 hours before the surgery. The operation will be performed in an ambulatory surgery center or in a hospital. You will be given anesthetic eye drops and monitored anesthesia care (MAC) to relax. You will be awake during the operation and you may notice light or movement.
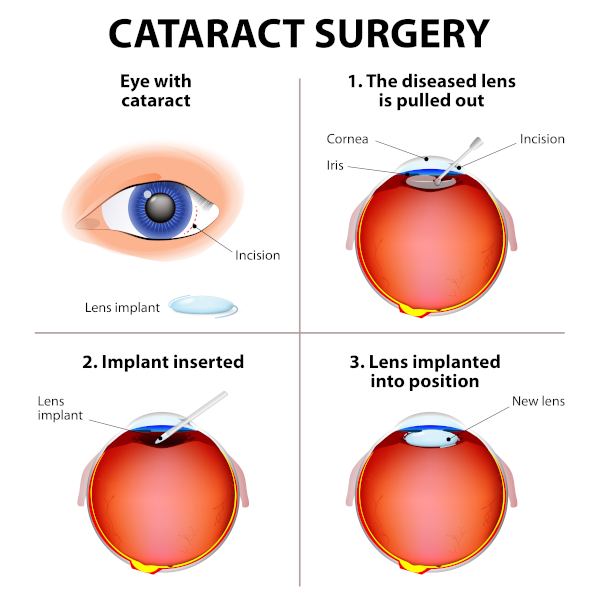
Then, using a special ophthalmic microscope, the surgeon Dr. Palioura will create tiny incisions in your cornea to insert a small ultrasound laser probe into the anterior chamber. Using the ultrasound laser probe the cloudy lens (cataract) will be dissolved into tiny pieces, which are then aspirated through the probe. After removing the cataract, the artificial intraocular lens will be implanted. The intraocular lens is inserted through the same small initial incision. This procedure significantly reduces the duration of visual recovery while reducing the risk of bleeding, scarring and irritation. Because of its small size, the incision can heal on its own only with the postoperative use of topical eye drops, without the need for injections or stitches.
At the end of the operation, a protective cover will be placed on your eye. When you recover from the anesthesia you will be ready to go home.
After the Surgery
For the first 4-6 weeks after the surgery, you will be using eye drops as directed by Dr. Palioura. Rubbing the operated eye should also be avoided.
For the first week avoid washing your eye with water and wear a protective shield or glasses when outside. Dr. Palioura will discuss with you in detail about when you can safely exercise again, drive or do other activities.
Benefits of Cataract Surgery
The benefits of cataract surgery are numerous and have been shown to significantly improve quality of life. Patients who have had successful cataract surgery experience several advantages in their daily life.
Better Quality of Vision

Patients have better quality of vision after cataract surgery, such as clearer images, brighter colors, and less difficulty with daily activities, such as night driving.
Greater Safety
Research shows that improved vision after cataract surgery reduces the chance of falls, making exercise, sports and hobbies safer. This results in improved physical health, richer social life and greater life expectancy.

Less Dependence on Glasses

After cataract surgery, many find that they no longer need to wear glasses or that their dependence on glasses is significantly reduced.
Sense of Confidence and Independence
Cataract surgery often leads to an increased sense of self-confidence and independence. Significant improvements have been reported even in patients with dementia or severe hearing loss.

Risks and Possible Complications of Cataract Surgery
Like any surgery, cataract surgery carries risks and potential complications, such as:
- Postoperative infection
- Bleeding
- Corneal edema
- Macular edema
- Retinal detachment
- Postoperative pain
- Loss of vision
- Dislocation of the intraocular lens (IOL)
Cataract surgery cannot restore vision that has been lost to other causes, such as macular degeneration, glaucoma, and diabetic retinopathy.
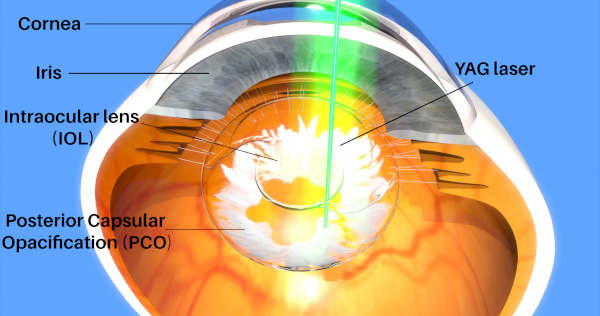
Posterior Capsule Opacification (PCO)
Your vision may become blurry weeks, months or years after cataract surgery. This is quite common and is called "posterior capsule opacification or PCO". Sometimes, the term "secondary cataract" is also used. It occurs when the membrane called the posterior capsule, which holds the intraocular lens in place, becomes opaque. Thus, if you notice blurry vision months or years after cataract surgery, you may need to have a simple laser procedure (YAG laser capsulotomy) to create an opening in the opacified posterior capsule and restore your vision.
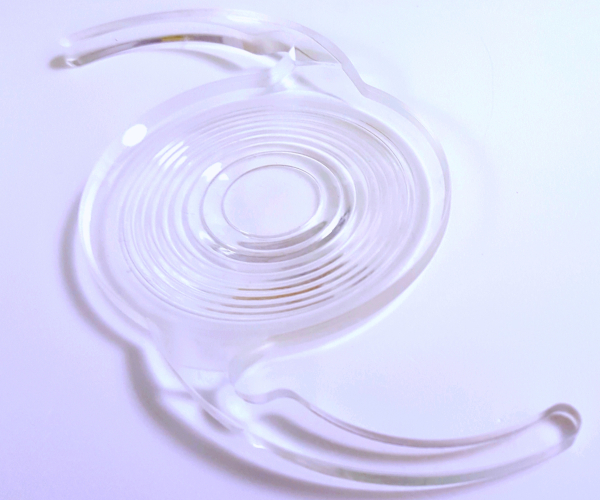
Intraocular Lenses (IOLs)

Intraocular lens (IOL) is the tiny artificial lens that replaces the natural lens of the eye after its removal during cataract surgery.
There are intraocular lenses with different focusing powers, as is the case with glasses or contact lenses. Dr. Palioura will measure the length of your eye and the curvature of your cornea and will calculate the power of the most suitable intraocular lens for you.
Most intraocular lenses are made of silicone or acrylic and have a coating to protect the eyes from the sun's harmful ultraviolet (UV) rays.
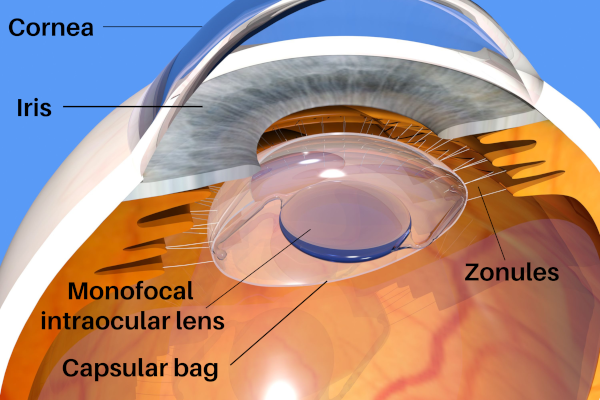
Monofocal Intraocular Lenses
The most common type of intraocular lens in cataract surgery is the monofocal one, which has a single focal point for either good near, intermediate or distance vision. Most people choose to have good long-distance vision and to wear glasses for reading or near work.
Toric Intraocular Lenses for Astigmatism Correction
Until recently, patients with astigmatism experienced a limited improvement in vision after cataract extraction and intraocular lens implantation. The patient with astigmatism would need additional surgery, such as LASIK, to fully correct his/her vision after cataract surgery. If the patient did not wish to undergo another surgery, the only option would be to use contact lenses or glasses to treat the astigmatism.
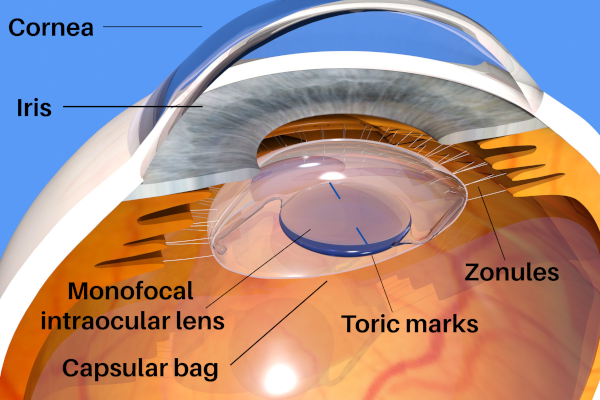
Toric intraocular lenses provide another option to patients with astigmatism, as they are specifically designed to correct astigmatism during cataract surgery. The choice of the lens is made after measurements of the curvature of the cornea (topography / tomography) and requires a special order. The lens is positioned in such a way that the notches on its surface are aligned with the axis of the patient's corneal astigmatism.
Multifocal and Extended Depth of Focus (EDOF) Intraocular Lenses for Presbyopia Correction
Until recently only monofocal intraocular lenses were available for implantation during cataract surgery. Patients with monofocal intraocular lenses can only focus on near or far objects, requiring glasses or contact lenses to see clearly at all distances.
Multifocal intraocular lenses allow for near, intermediate and distance vision correction, thus significantly reducing the need for glasses or contact lenses for most patients. Extended depth of focus (EDOF) intraocular lenses allow for intermediate and distance vision correction, thus limiting the need for glasses only for fine near vision tasks. Certain multifocal and EDOF intraocular lenses can also correct astigmatism. Implantation of a multifocal or EEDOF intraocular lens takes place at the end of cataract surgery.
Multifocal or EDOF intraocular lenses are not suitable for all patients. The decision to implant a multifocal or EDOF intraocular lens is made after specialized testing (topography / tomography of the cornea, optical coherence tomography of the macula) and discussion with Dr. Palioura to determine each patient’s needs.
N.B. The text on this page has been modified from the AAO webpage.
Publications, Talks and Abstracts by Dr. Palioura on Cataract Surgery
- Palioura, S., Ginat, D.T., Farrokh-Siar, L., Yanoga, F., Chodosh, J. (2014) Imaging after cataract and intraocular lens implant surgery. In Post-treatment Imaging of the Orbit, eds. Ginat, D.T., Freitag, S., Springer Science, Heidelberg, Germany.
- Palioura, S., Chodosh, J., Hart, L., Capaccioli, K., Ginat, D.T., Freitag, S.K. (2014) MRI, CT, and UBM imaging after corneal and cataract surgery. Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting, Orlando, FL, USA.
- Palioura, S., Chodosh, J., Hart, L., Capaccioli, K., Ginat, D.T., Freitag, S.K. (2014) MRI, CT, and UBM imaging after corneal and cataract surgery. The New England Ophthalmological Society (NEOS) Annual Meeting, Boston, MA, USA.
- Yesilirmak, N., Palioura, S., Yoo, S.H., Donaldson, K. (2015) Accuracy of intraoperative wavefront aberrometer for toric IOL in post-refractive eyes undergoing cataract surgery. Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting, Denver, CO, USΑ.
- Yoo, S.H., Palioura, S., Diakonis, V.F. (2015) IOL refractive surprises. In Intraocular Lens Surgery: Selection, Complications, and Complex Cases, eds. Randleman, B., Ahmed, I., Thieme Medical Publishers, New York, NY, USA.
- Palioura, S. (2015) Toric Intraocular Lenses for Keratoconus. The 29th International Congress of the Hellenic Society of Intraocular Implant and Refractive Surgery, Athens, Greece.
- Yesilirmak, N.*, Palioura, S.*, Culbertson, W., Yoo, S.H., Donaldson, K. (2016) Intraoperative wavefront aberrometry for toric intraocular lens placement in eyes with a history of refractive surgery. Journal of Refractive Surgery 32(1):69-70.
- Palioura, S., Yesilirmak, N., Culbertson, W., Yoo, S.H., Donaldson, K. (2016) Intraoperative wavefront aberrometry for toric intraocular lens placement in eyes with a history of refractive surgery. The American Society of Cataract and Refractive Surgery (ASCRS) Annual Congress, New Orleans, LA, USA.
- Vavvas, D.G., Dryja, T.P., Wilson, M.E, Olsen, T.W., Shah, A., Jurkunas, U., Pineda, R., Poulaki, V., Palioura, S., Veldman, P., Tsilimbaris, M., Rhee, D., Colby, K., Hunter, D.G., Thanos, S., Sakamoto, T., Pasquale, L.R., Miller, J.W., Vanderveen, D., Lambert, S.R. (2018) Doubts about spontaneous lens regeneration after cataract surgery. Nature 556(7699):E2-E3. doi: 10.1038/nature26149.
- Palioura, S., Relhan, N., Leung, E., Chang, V., Yoo, S.H., Dubovy, S.R., MD, Flynn HW Jr. (2018) Delayed-onset Candida parapsilosis cornea tunnel infection and endophthalmitis after cataract surgery: histopathology and clinical course. American Journal of Ophthalmology Case Reports 11:109-114.
- Palioura, S. (2018) Technological innovations in cataract surgery. Best of the American of Ophthalmology Annual Meeting, Athens, Greece.
- Palioura, S., Relhan, N., Leung, E., Chang, V., Yoo, S.H., Dubovy, S.R., Flynn, H.W. Jr. (2019) Delayed-onset Candida parapsilosis cornea tunnel infection and endophthalmitis after cataract surgery: histopathology and clinical course. The XVI Biannual Aegean Retina Meeting, Mykonos, Greece.
- Kondylis, G., Klavdianou, O., Palioura, S. (2019) Multifocal and extended depth of focus intraocular lenses. Annals of Eye Science 4:5.
- Palioura, S., Relhan, N., Leung, E., Chang, V., Yoo, S.H., Dubovy, S.R., Flynn, H.W. Jr. (2019) Delayed-onset Candida parapsilosis cornea tunnel infection and endophthalmitis after cataract surgery: histopathology and clinical course. The 36th Annual Congress of the European Society of Cataract and Refractive Surgery, Paris, France.
- Palioura, S. (2019) Clinical Questions in Ophthalmology. Annual Meeting of the Ophthalmological Society of Central Greece, Larisa, Greece.
- Palioura, S. (2019) Cost-Benefit Analysis of Single Versus Repeated Use of Medical Devices in Cataract Surgery. The 2019 Alcon Innovative Technology Summit, Athens, Greece.
- Venkateswaran, N., Amescua, G., Palioura, S. (2020) Perioperative management of dense cataracts. International Ophthalmology Clinics 60(3):51-60.
- Naoum, P., Palioura, S., Naoum, V., Nomikos, N., Bachtalia, K., Zisis, K., Athanasakis, K., Kyriopoulos, J. (2021) Cost-benefit analysis of single versus repeated use of single-use devices in cataract surgery. Clinical Ophthalmology 15:1491-1501.
- Palioura, S. (2021) Cataract Surgery in Patients with Fuchs’ Endothelial Dystrophy. The 35th International Congress of the Hellenic Society of Intraocular Implant and Refractive Surgery, Thessaloniki, Greece.
- Palioura, S. (2021) Cataract Surgery in Patients with Keratoconus. The 54th Annual Congress of the Hellenic Ophthalmological Society, Volos, Greece.
- Giachos, I., Trichonas, G., Palioura, S. (2022) Implantation of high-power intraocular lenses in a patient with nanophthalmos and very low axial length (AL < 16.50 mm). The 17th Annual Congress of the Greek Vitreoretinal Society, Athens, Greece.
- Palioura, S., Trichonas, G. (2022) Cataract surgery and implantation of high-power (57 D) intraocular lenses in a patient with nanophthalmos (AL < 16.5 mm). The American Society of Cataract and Refractive Surgery Annual Meeting, Washington D.C., USA.